Something I’ve noticed: when people start looking into GLP-1’s, retatrutide gets all the attention.
It has more hype, more buzz, and more of that “this is the future” energy than tirzepatide.
But when you actually look into the data, the answer isn’t so obvious.
Tirzepatide: The Case For It
Tirzepatide is a dual GIP + GLP-1 agonist. It hits two receptor pathways simultaneously.
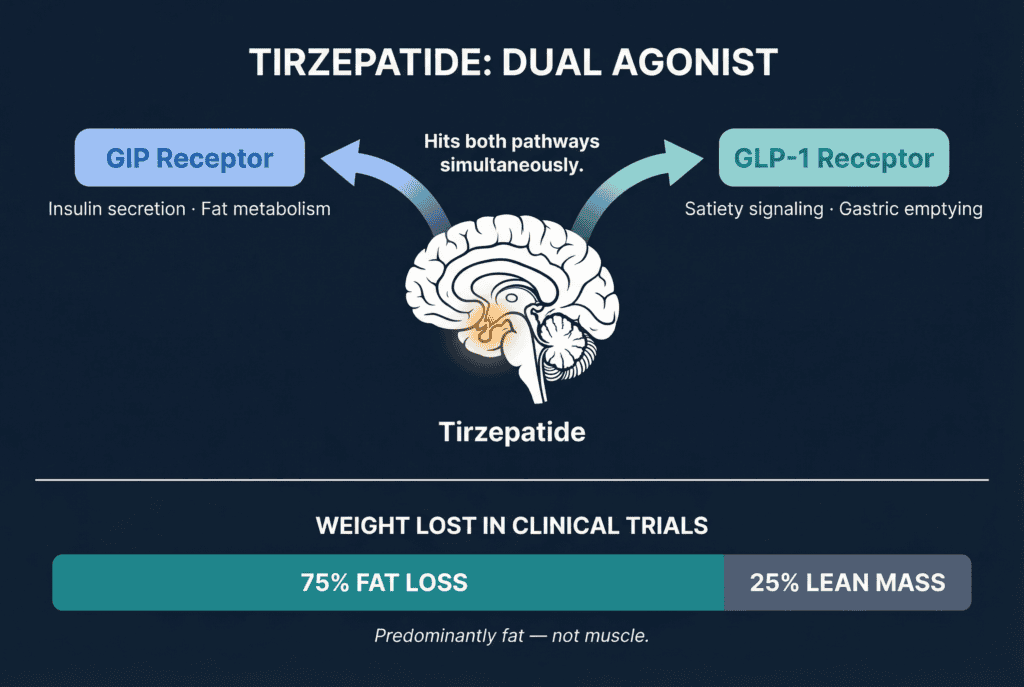
That GIP pathway is key. It plays a direct role in nutrient partitioning. Directing calories toward muscle glycogen storage rather than fat, and it has documented anti-catabolic effects on skeletal muscle.
In clinical trials, roughly 75% of weight lost was fat, with about 25% coming from lean mass.
But it’s important to understand what that actually means.
“Lean mass” doesn’t just mean muscle. It includes water, glycogen, and everything that isn’t fat. And most people in these studies aren’t lifting hard or eating enough protein, which naturally skews that number higher.
In a properly structured cut, with adequate protein and heavy training, you can maintain virtually all of your muscle while losing fat.
So a 75/25 split in the general population is actually solid. And in the right setup, it can be even better.
It’s also been FDA-approved since 2022.
There’s 72 weeks of clinical trial data, a well-characterized side effect profile, and it’s widely available through compounding pharmacies at a fraction of the brand-name price.
It’s the proven compound.
Retatrutide: Why More Isn’t Always Better
Retatrutide is a triple agonist. It adds Glucagon receptor activation on top of GIP and GLP-1.
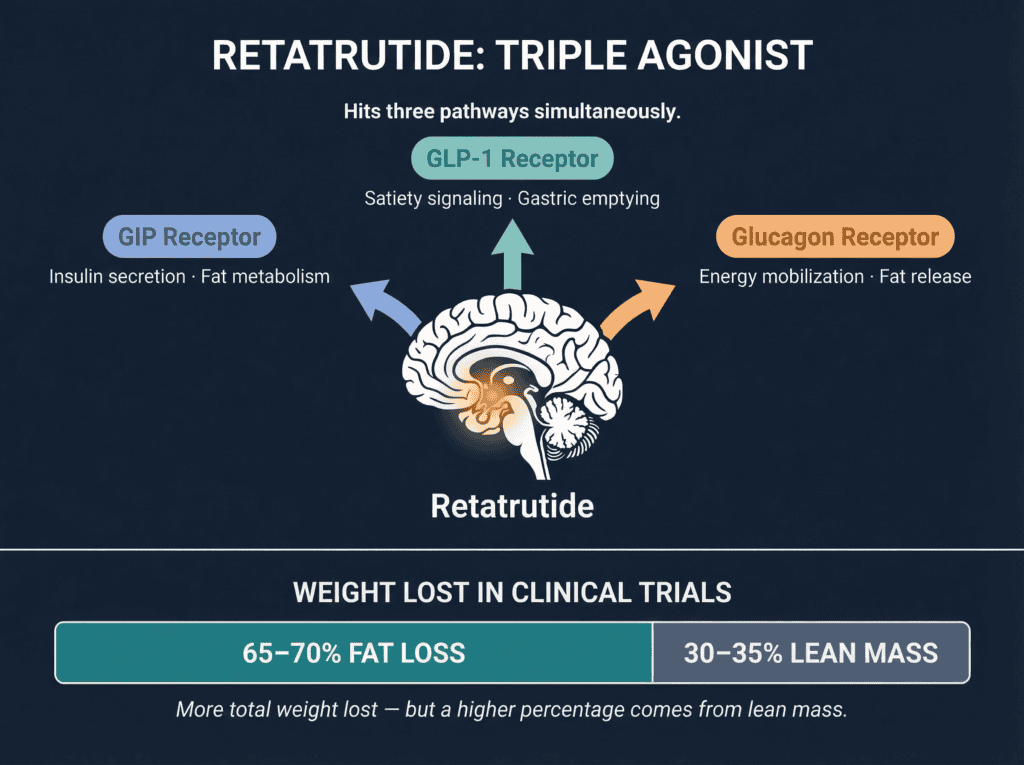
Most people know glucagon as the opposite of insulin. Insulin stores energy. Glucagon releases it. It raises your heart rate and signals the body to mobilize stored energy from both fat and muscle.
What’s hilarious is that most people think the glucagon pathway is what helps you keep your muscle… and that reta is better for muscle.
Literally everyone thinks this.
I feel like I’m taking crazy pills, lmao.
Because glucagon is NOT an anabolic pathway! It is a catabolic pathway…
Here’s what the data shows.
Yes, at maximum dose it produces slightly more weight loss. About 24 lbs for every 100 lbs of body weight, versus 20-22 lbs on Tirzepatide
But here’s the problem with that third receptor.
- Retatrutide’s fat-to-lean ratio runs roughly 65-70% fat, 30-35% lean mass.
- Tirzepatide edges it at 75% fat and 25% lean mass.
The difference isn’t dramatic, but it’s real, and it goes in the wrong direction.
When you’re already fighting to protect muscle during a cut, there’s no reason to choose the compound with the slightly worse ratio.
This is even riskier as you drop into the single-digit body fat range.
The leaner that you get, the more prone you are to lose muscle mass. Retatrutide is probably okay if you have a lot of weight to lose, but not worth it if you want to get really lean.
And the muscle issue is just one part of it.
- Heart rate increases of +4-7 bpm, versus +1-3 bpm with Tirzepatide
- Likely decreased heart rate variability (HRV)
- Potentially disrupted sleep quality
For a performance-oriented person who trains hard, prioritizes recovery, and tracks HRV? Those trade-offs are not trivial.
Plus it’s not FDA-approved. It’s still in Phase 3 trials. Long-term safety data are limited.
Note: If you go on a low enough dose of Retatrutide, you can avoid hitting too high of a deficit and mitigate the significant heart rate increase. But this isn’t ideal. I posted about this on X yesterday morning…
The real advantage of Tirzepatide is control.
It gives you one dial: appetite. You can adjust your deficit precisely without introducing a second variable like increased energy expenditure and elevated heart rate.
If your goal is maximum weight loss, retatrutide makes sense.
But if your goal is to get lean while preserving muscle and minimizing unnecessary stress on your system, tirzepatide is the better tool.
My Choice
Tirzepatide wins.
It’s the smarter call.
- FDA-approved
- Extensively studied
- Muscle-sparing
- Well-tolerated
- Widely available
It’s the compound I chose for my own protocol. And it’s the compound we’re making available through Kino Clinic.
If you want medically supervised access to compounded Tirzepatide, with a real protocol built around protecting your physique, this is it.
Talk soon,
Greg O’Gallagher